
Birth Education: Know Your Rights & Options (Hospital Edition)
An excerpt from Birthing While Black: A Hospital Guide 🖤

This piece in an excerpt from our print zine, Birthing While Black: A Hospital Guide, created in partnership with the BLACK Wellness and Prosperity Center in California, Tre Borden /Co and the James Irvine Foundation. The zine is NOW shipping!
Understanding your rights, your options and your body’s innate wisdom is one of the strongest ways to prepare for the life altering passage of birth. Education won’t guarantee a specific outcome, but it will help you move through the experience with more clarity, confidence and calm.
Physiological Birth vs. Medicalized Birth
A physiological birth is one that follows the body’s natural rhythms and hormonal cues, typically involving spontaneous labor, minimal technological interference, labor companionship and a focus on the parent’s instincts and comfort. It also includes things like skin-to-skin contact with baby and delayed cord clamping immediately postpartum.
When uninterrupted, your body releases a carefully choreographed cascade of hormones — like oxytocin, endorphins and prolactin — that help labor progress, ease pain and support bonding with your baby. But these hormones are sensitive. High stress levels and spikes in cortisol can interfere with this natural flow, stalling labor or increasing the need for intervention. That’s why emotional safety and a calm environment aren’t just “nice to have” — they’re essential to supporting physiological birth. Practices like dim lighting, quiet surroundings and skin-to-skin contact with baby (along with delayed cord clamping) can help preserve this delicate hormonal dance and ease the transition into postpartum.
A medicalized birth involves more clinical oversight and reliance on procedures, medication and technology — like inductions, epidurals or continuous monitoring — which may be helpful or necessary depending on the situation, but aren’t always tailored to individual needs.
There are also hybrid approaches, where physiological processes are supported within a medical framework. Many births fall somewhere along this spectrum.
Keep in mind, hospitals are designed for clinical care — which means their routines and protocols can sometimes make a physiological birth more difficult to achieve. If you’re aiming for an unmedicated or low-intervention birth, it’s important to find a provider and location aligned with that vision. Some hospitals offer midwifery-led care or birth center-style options within their system. And while hospital staff may rotate, a dedicated doula can offer support that centers your voice throughout the process.
Not every body or pregnancy will allow for a fully physiological birth — and that’s okay. You might feel a sense of disappointment or loss around that, and that’s valid too. You deserve care that honors both your reality and your emotional experience.
And if physiological birth is an option, but not aligned with your birth vision, your choice also deserves respect and support.
Birth is deeply personal. Even with the same parents, no two births look the same. The goal is to be well-informed — not rigid. Talk with your trusted provider about your hopes, and work together to explore what’s realistic for you.
Whatever path feels right for you, we encourage taking a birth education course that aligns with your values and vision. It will help you understand what’s happening in your body, explore your options; and ask meaningful, educated questions as you prepare for birth.
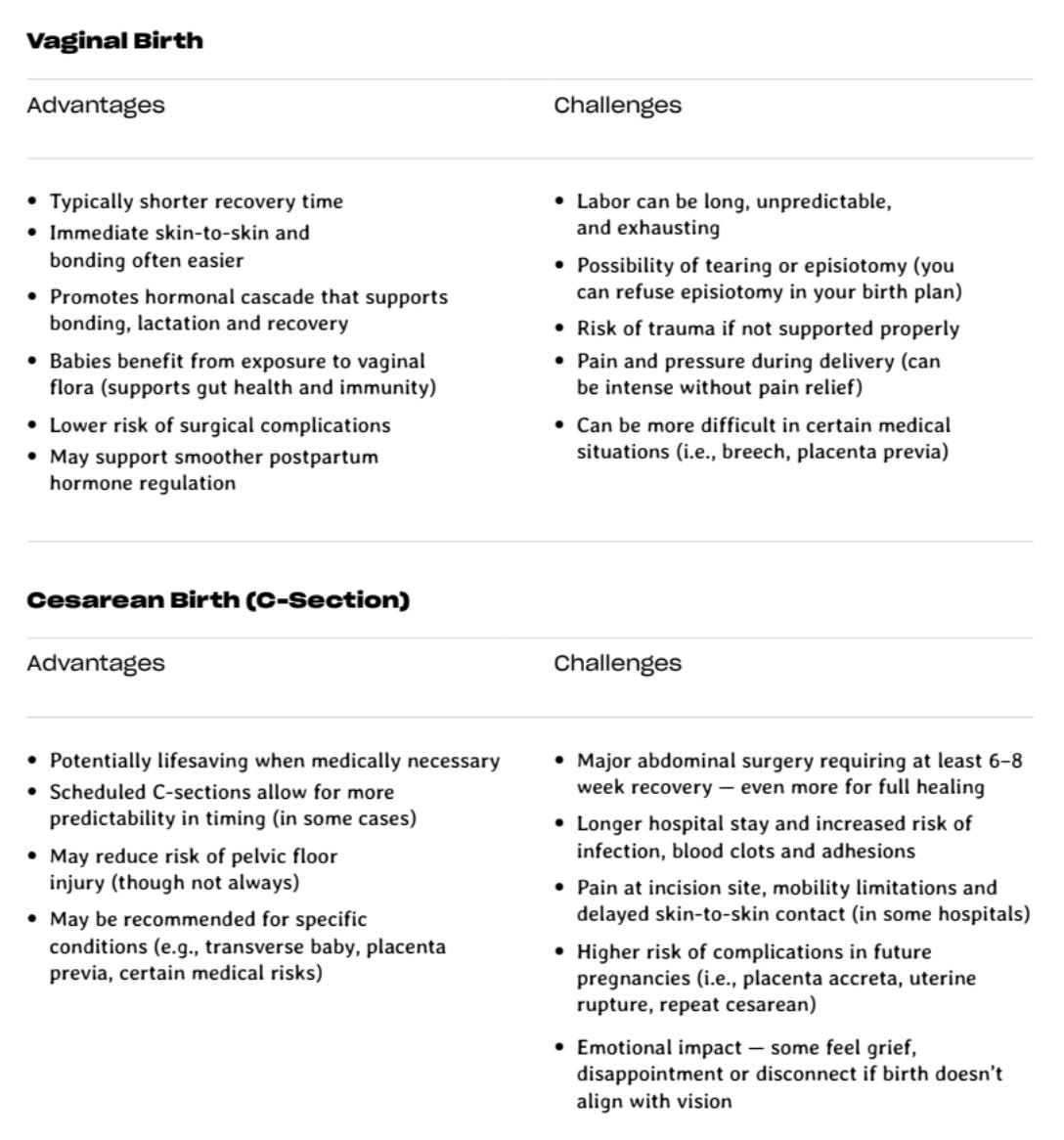
Cesarean vs. Vaginal Birth
In the U.S., more than 30% of births happen by cesarean section — a surgical procedure that delivers your baby through incisions in the abdomen and uterus. That’s twice the rate recommended by the World Health Organization, and rates are even higher for Black women. C-sections can be life-saving — but they’re also major surgery, with longer recovery times and higher risks in future pregnancies. Too often, they’re offered for reasons like scheduling convenience or liability concerns, not true medical need.
Cesarean birth is sometimes presented as the “easier” option or a way to bypass the pain of labor. While it may offer more predictability, it also involves major abdominal surgery — and recovery begins while you’re caring for a newborn. Too often, the full risks and long-term considerations aren’t clearly explained. We believe you should have the whole picture.
In a system that doesn’t always center our individual outcomes, it’s essential to understand our options. Vaginal birth is not always possible, but when it is, it can support faster recovery, hormonal regulation and early bonding. The most important thing is being informed — and choosing the path that supports your health, your baby and your healing.
And if you’ve had a previous cesarean, know this: a vaginal birth after cesarean (VBAC) may still be possible. While some providers say, “once a C-section, always a C-section,” that’s not always true. VBACs can be safe and even redemptive — and you deserve to know if it’s a medically safe option for you.
High-Risk Pregnancy
A pregnancy is typically labeled high-risk when certain conditions or circumstances increase the likelihood of complications for the parent or baby. This designation often means you’ll require more frequent monitoring, additional testing or the care of a specialist — and for many, a hospital birth becomes the recommended or required setting.
Common high-risk factors include:
Chronic high blood pressure (hypertension or preeclampsia)
Gestational diabetes (especially if uncontrolled)
Type 1 or Type 2 diabetes
History of preterm labor or preterm birth
Placenta previa or placental abruption
Multiple gestation (twins or more)
Breech or transverse baby position (at term)
Advanced maternal age (35+)
Teen pregnancy (under 17)
Prior cesarean section or uterine surgery
History of stillbirth or pregnancy loss
Autoimmune disorders (i.e., lupus)
Kidney or liver disease
Clotting disorders or history of thrombosis
Obesity (depending on BMI and associated risks)
Fetal growth restriction (IUGR)
Rh incompatibility
Substance use disorder
Certain infections (e.g. HIV, active herpes, toxoplasmosis)
Severe anemia or other blood disorders
That said, not all “high-risk” labels are created equal. Some conditions — like breech presentation or gestational diabetes — may still allow for an out-of-hospital birth depending on your provider’s training, your state’s laws, and how well the condition is managed. Some highly skilled midwives can safely attend breech or twin births, though this is increasingly rare and requires specialized experience.
In other cases, the risk level may be exaggerated due to outdated policies or provider preferences. For example, some hospitals classify VBACs (vaginal birth after cesarean) as high-risk by default, even though research supports VBAC as a safe option for many. Similarly, “advanced maternal age” is not a diagnosis — and while it may warrant additional monitoring, it does not automatically rule out the possibility of a healthy, low-intervention birth.
This is why informed decision-making matters. Ask questions. Understand the reasons behind any “high-risk” designation. Every body is different. Every provider is different. And every state has different laws that determine who can legally support what kind of birth.
You may find that your care options are limited — but you may also find that a trusted provider is willing to work with you to safely manage your care, rather than automatically funneling you into a surgical or highly medicalized path. Knowing the difference is key.
Pain Relief: Epidural Block
An epidural block (typically referred to as simply “an epidural”) is a regional anesthetic injected into the lower spine to block pain from the waist down. It’s the most common form of labor pain relief in the U.S., used in 70–80% of births. You’ll find more regional pain relief options below, in the Alternative Pain Relief section.
For many, an epidural offers significant relief — allowing rest during long labors, reducing the intensity of contractions, and helping some parents feel more present or grounded. But like any medical tool, it comes with trade-offs. Some side effects include:
Drop in blood pressure
Fever
Inability to urinate (may require catheter)
Shivering or itching
Longer pushing phase
Risk of spinal headache
Rare but serious risks like nerve injury or infection
Timing matters — placed too early (before active labor), it can increase intervention risk. Some hospitals offer “walking” epidurals, but they’re rare. Know this: an epidural isn’t bad or good. It’s a tool. Learn how it works, understand your options and decide what’s right for you.
Alternative Pain Relief Options in the Hospital
Pain in labor is real — but so are your options. No matter how you give birth — vaginally or by cesarean, with or without medication — you will experience some form of pain or discomfort. Whether it’s the intensity of contractions, the soreness of recovery, or the sting of a healing incision, pain is part of the process — not a failure or something to fear.
Pain is also information. It lets you know something is shifting. In labor, it’s a signal that your body is doing the work of bringing life forth. While medication can help manage it, it may also numb some of that awareness — and that’s something to weigh as you consider your options.
If you’re hoping to avoid or delay an epidural, ask your provider what tools your hospital offers. These may include:
Movement & Positioning
Walking, rocking, squatting or swaying
Using a birthing ball or peanut ball
Upright or hands-and-knees positions to reduce pain and support baby’s descent
Breathwork & Guided Relaxation
Deep breathing, visualization and vocalization can anchor you through contractions
Practice ahead of time — or ask your doula or nurse to guide you
Hydrotherapy
Laboring in a shower or tub can ease tension and offer natural pain relief
Some hospitals have tubs — ask and tour ahead of time
Heat & Cold Therapy
Warm compresses on the lower back or pelvis
Cold packs to reduce inflammation and soothe pressure points
Counterpressure & Massage
Applied to the lower back or hips during contractions (often by a doula or partner)
TENS Unit
A small device that delivers electrical pulses to block pain signals
Some hospitals allow them, some provide them — bring your own if needed
In addition to epidurals, hospitals may offer other medication-based options for managing labor pain, including:
Nitrous Oxide (Laughing Gas)
Inhaled through a mask to reduce anxiety and help manage pain perception. You control when to use it.
Side effects may include dizziness or nausea, but these wear off quickly. Safe for most birthing parents and babies.
Systemic Analgesia (Opioids)
Given by IV or injection to “take the edge off” without full numbness or unconsciousness.
Can cause drowsiness, nausea or (in high doses) breathing issues; may affect baby’s alertness and early breastfeeding.
Local Anesthesia (Pudendal Block)
Numbs the vaginal, vulvar and perineal area with an injection; often used just before delivery or for repair.
Minimal effect on baby; rare risks include allergic reaction or nerve issues if overdosed.
Regional Pain Relief (Spinal Blocks & Epidural Blocks)
A spinal block is a one-time injection into spinal fluid for fast, full pain relief — commonly used for C-sections; wears off in 1–2 hours.
A CSE Block (Combined Spinal–Epidural) combines immediate relief from a spinal with long-lasting pain control via epidural; uses lower medication doses for similar effect.
Both options have the same side effects and risks as an epidural block.
General Anesthesia
Medications given through IV or injection to reduce pain perception. Induces unconsciousness for rapid pain relief — used mainly in emergencies, like urgent C-sections.
Risks include aspiration, breathing issues and newborn drowsiness or low breathing rate after birth.
There’s no one “right” way to manage labor pain. Every person has different thresholds, histories and medical needs. What matters most is knowing, researching and discussing your options, listening to your body and feeling supported in whatever decisions you make along the way.
Pre-Existing Conditions & Prenatal Care
If you have a medical condition like hypertension, diabetes, fibroids or a previous cesarean, prenatal care becomes even more important. Learn how your condition(s) may affect labor and birth and what steps can reduce risk. This is a great topic to bring up when choosing your midwife or OB, so you can plan ahead and avoid unexpected decisions down the line. The right provider will help you understand your options — not scare you into submission.
One starting point to consider is the Preconception Medical Assessment (PreMa), a tool that can help you identify potential risks so you can shape a personalized care plan early on.

Common Hospital Interventions & Alternatives
In birth, an intervention is any action or procedure used to monitor, manage or alter the natural course of labor and delivery. Some interventions are necessary and lifesaving. Others may be routine, policy-driven, or offered out of habit — not because something is wrong.
Common interventions in hospital births include:
Continuous electronic fetal monitoring (EFM)
Labor induction (using medications like Pitocin or procedures like membrane stripping)
Artificial rupture of membranes (breaking your water)
Epidural anesthesia
IV fluids and restrictions on food and drink
Limited mobility during labor
Vaginal exams to check cervical dilation
Episiotomy
Vacuum or forceps-assisted delivery
Cesarean section (C-section)
Immediate cord clamping
Separation of baby and parent for routine procedures
Definitions for each of these can be found in the glossary. Some may be medically necessary — but others may be offered out of routine, policy or habit. Learn what each intervention is, when it’s truly indicated, and which interventions are optional. The more informed you are, the better prepared you’ll be to navigate decisions with confidence and clarity — even in the moment.
Your Legal Rights in a Hospital Birth
Generally speaking, you have the legal right to:
Be fully informed about your care
Refuse or consent to any procedure
Ask questions — and receive answers you understand
Have a support person with you
Access your medical records
These rights don’t disappear when you walk into a hospital. But in the intensity of labor — or the speed of medical decision-making — they can be easily overlooked if you don’t know them ahead of time.
Informed consent is more than a signature on a clipboard. It’s a process — one that requires your provider to explain, in language you understand:
What the proposed procedure is
Why it’s being recommended
What the risks and benefits are
What alternatives exist (including doing nothing)
You then have the right to take that information, ask questions, weigh your options and make the decision that feels right for you.
You also have the right to informed refusal — meaning you can decline any procedure you do not consent to. That includes interventions like cervical checks, Pitocin, membrane sweeps or even cesareans — unless your life is in immediate danger and you are physically or mentally unable to consent (more on that below).
Exceptions to informed consent: In rare, truly emergent situations — such as if you are unconscious, lose decision-making capacity, or require a life-saving intervention immediately — a provider may act without explicit consent under the principle of implied consent to preserve life or prevent permanent harm. Even then, they are ethically expected to honor your documented wishes and known values wherever possible. This is where an aligned birth partner and doula becomes essential — someone who knows your plan, can advocate clearly in the moment, and help ensure your preferences are respected even when you can’t speak for yourself.
Bottom line: You are not obligated to comply with everything suggested. You can always ask, “Is this urgent or can we talk about it?” or “What happens if I wait or say no?” Staying curious and clear about your rights is not being difficult — it’s being informed.
Using the BRAINS Framework
When you’re faced with a decision in labor, the BRAINS acronym can help you slow down and explore your options:
B — What are the Benefits?
R — What are the Risks?
A — Are there Alternatives?
I — What does your Intuition say?
N — What happens if we do Nothing right now?
S — Ask for Space or Support if needed.
This tool can help you stay centered and collaborative, even in moments that feel rushed. You can use it yourself, or your birth partner or doula can help guide the conversation using these prompts.
How Hospital Policies Shape Care — and How to Navigate Them
Hospitals are governed by policies that aim to streamline care, manage liability and standardize procedures — but they don’t always leave room for individual preferences. Routine protocols (like limiting movement after epidurals, or restricting food intake during labor) may be framed as non-negotiable, even when there’s room for flexibility. Visiting hours, mandatory monitoring and documentation requirements can also influence how supported or restricted you feel.
Here’s the truth: policies aren’t always laws. You can ask questions, request exceptions and push back respectfully. This is where preparation pays off — knowing your rights, having your preferences documented and choosing providers and support people who will advocate for your care plan. When something doesn’t feel right, it’s okay to ask, “Is this a policy or a preference? Is there any flexibility?” Respectful self-advocacy is a skill — and you don’t have to do it alone.
The magazine looks really beautiful and this is so important and well written, it made me realize I have some trauma around my last birth which was in a hospital. What happened to me was that after my baby's head was already out, one of the nurses pulled his shoulders out. My husband told her not to, but the damage was already done.
I didn't need help. My body was already pushing him out fine, and the hardest part was the part I'd already done.
I've never seen this particular intervention mentioned anywhere. I'm not sure how common it is or if other people are just not bothered by it, but even in my first hospital birth, which was very traumatic, they didn't pull my baby out of me.
I had to fight on a lot of things in both births and I have no problem doing that since I have been lucky enough to go in fairly prepared each time, but I wasn't prepared for that.
Please provide the link!
Thank you!
Thank You!!
Thank YOU!!!